Ulnar Collateral Ligament Injury (UCL)
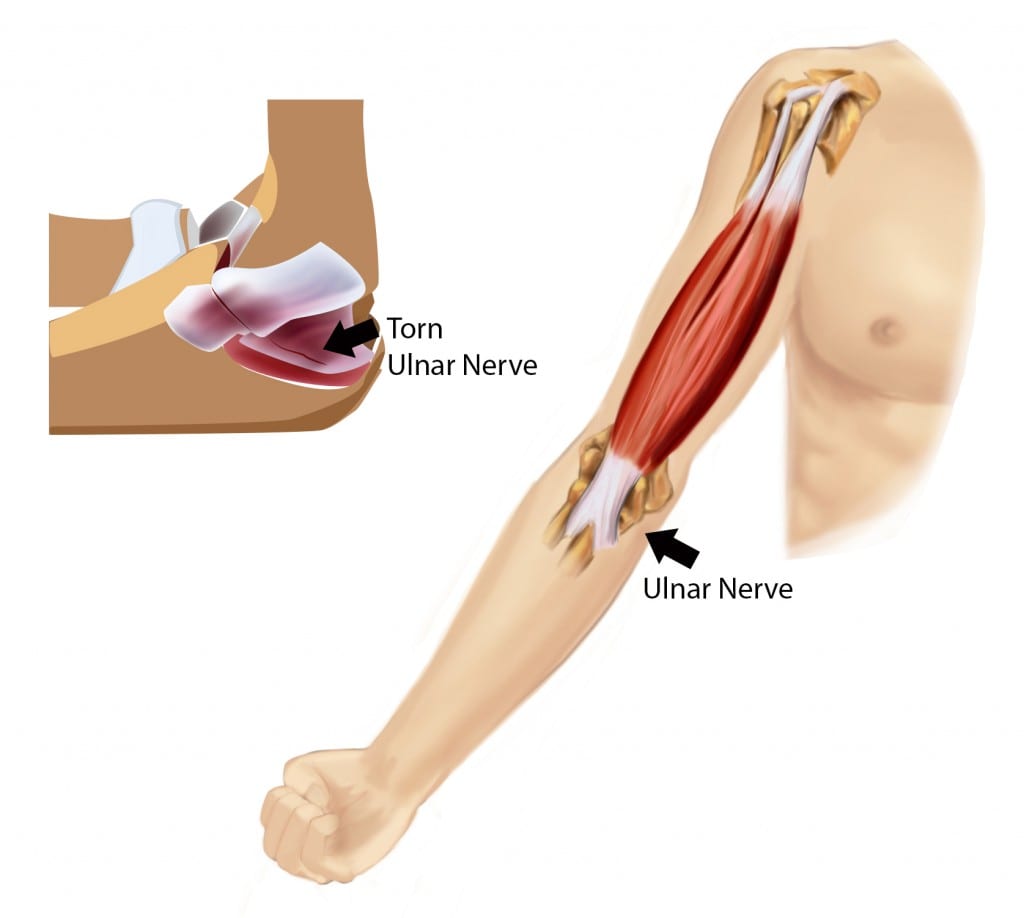
The elbow joint is made of three bones, the long arm bone (humerus) and the two forearm bones (ulna and radius). The elbow joint works like a hinge. The humerus creates the base of the hinge and the olecranon of the ulna rotates nearly 150 degrees around the hinge. The rotation allows for elbow flexion and extension. As the elbow is straightened, the stability of the joint on the inner and outer sections is protected by ligaments that attach bone to bone. The ulnar collateral ligament (UCL) is on the inside of the elbow joint, near the body when the palm is rotated up. It protects the elbow from outward strain that would pull the forearm out of alignment with the humerus.
This content was created using EBSCO’s Health Library
A traumatic strain to the ulnar collateral ligament is most likely to occur during athletic activities. When a player falls on an outstretched arm that is relatively overhead, the first thing that hits the ground may be the upper forearm. A repetitive strain to the UCL may be caused by repeated overhead reach while hitting a ball. When the arm is nearly straight at the elbow and the hand hits a ball, it can put specific sprain on the inside of the elbow joint. The ligament may endure light but repetitive strains over a period of time and eventually stretch beyond its normal length. As the ligament stretches, it becomes less supportive of the elbow joint and can lead to arthritis at the elbow joint (because the poor alignment will cause the joint surfaces to rub) or to a full-thickness tear
This content was created using EBSCO’s Health Library
Factors that increase your risk of Ulnar Collateral Ligament Injury Include:
- Overhead Athlete
- Athlete in heavy sports
- Performs repetitive overhead activities
- Quantity of pitches thrown and form of pitches
This content was created using EBSCO’s Health Library
Symptoms include:
- Feeling of a snap or pop
- Swelling in the joint
- Smooth glide of the elbow from extension to flexion will be painful and unstable
This content was created using EBSCO’s Health Library
The doctor will ask about your symptoms and medical history. You may also be asked about your recent physical activity. Your visit may also include:
- A valgus stress test
- Musculoskeletal ultrasound
- An MRI or X-Ray
This content was created using EBSCO’s Health Library
Therapy following a non-surgical UCL injury will focus on regaining active range of motion of the elbow, providing education on avoiding additional strain and using progressive strengthening techniques to improve the muscular stability around the joint. Active motion will be dependent on whether there were other injuries to the elbow that might prevent motion at the hinge joint. Education on avoiding additional strain include the use of elbow braces during heavy activity, reducing force against the arm in full weight bearing (as in pushups or bench press), and protecting the elbow during ball play. The therapist will likely begin a strengthening program to the triceps and biceps muscles as well as the rotator cuff muscles in order to protect the elbow and shoulder in overhead activity. It may take 3-6 months to return to sport following a mild to moderate strain. With a post-surgical UCL injury, the elbow may be casted for 10-12 days. During that time, the therapist will provide education on light exercises to the shoulder and hand to do while the elbow is casted. Therapy will focus on reducing the atrophy of the muscle during casting, often times introducing isometric exercises that can be done inside the cast. The “Tommy John” surgery is a repair of an UCL due to strain or tear caused mainly by pitching activities. Once a UCL repair has been performed, the return to sport may be closer to 16-18 months.
This content was created using EBSCO’s Health Library
To prevent an ulnar collateral ligament strain you should perform a progressive stretch and strength program before all sports activities. If you are involved in heavy sports or repetitive activities that will strain the elbow, wear a protective sleeve or brace that gives the UCL support. Seek the attention of a physician or physical therapist when you suspect an injury.
This content was created using EBSCO’s Health Library
- Edwards H, Smith D. Sideline assessment and return-to-play decision-making for an acute elbow ulnar collateral ligament sprain. Inj J Sports Phys Ther;8(2);212-5.
- Ellenbecker TS, Wilk KE, Altchek DW, Andrews JR. (2009). Current concepts in rehabilitation following ulnar collateral ligament reconstruction. Sports Health;1(4):301-313.
- Eygendaal D, Rahussen FT, Diercks L. (2007). Biomechanics of the elbow joint in tennis players and relation to pathology. Br J Sports Med;41(11):820-823.
- Langer P, Fadale P, Hulstyn M. (2006). Evolution of the treatment options of ulnar collateral ligament injuries of the elbow. Br J Sports Med;40(6):499-506.
- Rodriguez-Martin J, Pretell-Mazzini J, Andrew-Esteban EM, Larrainzar-Garigo R. (2011). Outcomes after terrible triads of the elbow treated with the current surgical protocols: A review. Int Orthop;June;35(6):851-860.
- Wilk KE, Macrina LC, Cain EL, Dugas JR, Andrews JR. (2012). Rehabilitation of the overhead athlete’s elbow. Sports Health; Sept;4(5):404-411.
This content was created using EBSCO’s Health Library