Cubital Tunnel Syndrome
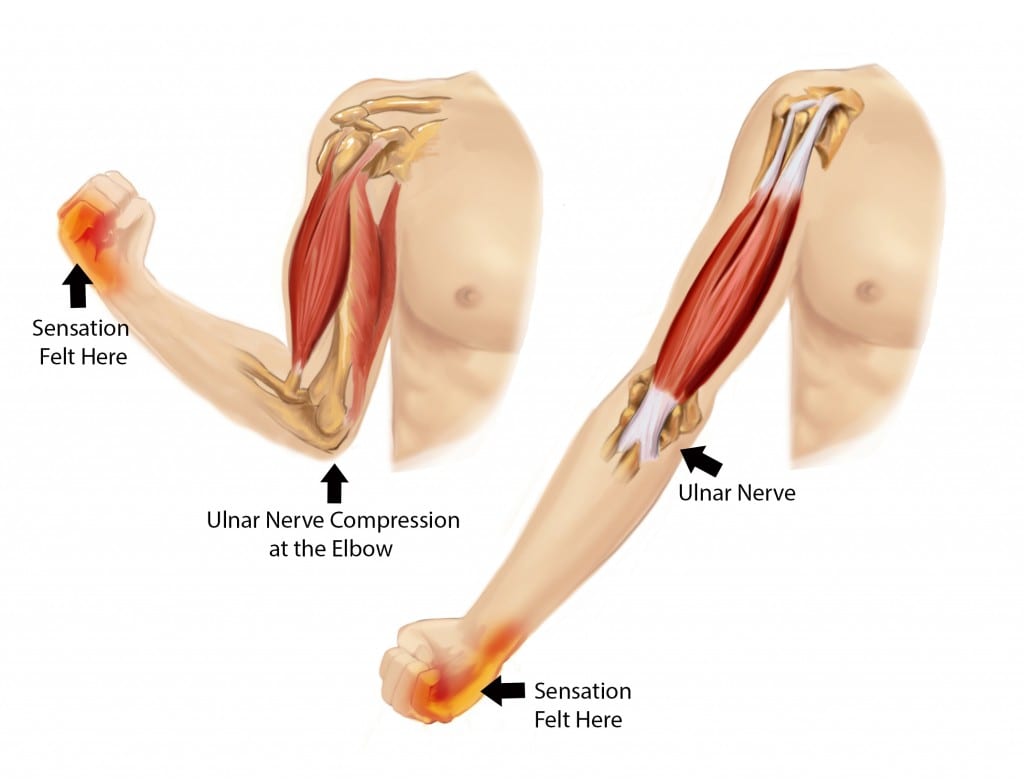
Cubital tunnel syndrome refers to a compression of the ulnar nerve at the elbow. The ulnar nerve is a combination of nerves that originates at the neck and travels to the pinky side of the hand. The nerve is both motor and sensory and provides both the motor control and the sensation to the pinky and the side of the ring finger. It also provides muscle control to the small muscles in the hand that provide fine motor coordination in tip and pinch. Handwriting can be significantly affected by ulnar nerve dysfunction.
The ulnar nerve can be compressed at multiple sites in the arm and will be evaluated for specific compression at the elbow before treatment can begin. The physician use a nerve conduction study to evaluate for nerve latency, or the amount of time that it takes for the nerve to send an electrical signal past the compression spot and toward the hand. If the affected side is slower than the unaffected side, the diagnosis of cubital tunnel syndrome may be appropriate.
50% of cases resolve without surgical intervention
Clinical evaluation techniques may be falsely positive in up to 24% of cases.
Cubital tunnel symptoms may actually be related to compression at the neck
65% of cases occur in women
Average age of diagnosis is 52 years of age. Patient age is the most important factor in determining if surgery is needed to improve the condition.
This content was created using EBSCO’s Health Library
There may be multiple causes of cubital tunnel syndrome:
- Repetitive strain: Repetitive bending of the elbow or sustained bending of the elbow causes the ulnar nerve to bend at a maximum of 150 degrees. When the elbow is bent to hold a phone to the ear, the nerve may be bent for a long period of time.. When the nerve is pinched repetitively, it can become inflamed and drag through the tunnel that houses it.
- Direct compression: When the elbow has direct pressure to the ulnar nerve, it can cause the same amount of pinch as when the elbow is bent. Compression may occur when the elbow is pushed onto a table during computer work, when a shirt sleeve is pushed up to the elbow, or when an elbow strap is used for tennis elbow.
- Trauma: Trauma to the elbow may cause a fracture or injury that affects the cubital tunnel. An x-ray may be used to determine whether the cause for the compression is a bony fragment.
This content was created using EBSCO’s Health Library
- Repetitive use of upper limbs that require the bending of the elbow
- Prior Injury to the elbow
- Bone Spurs at the joint
This content was created using EBSCO’s Health Library
The primary complaint in cubital tunnel syndrome is the feeling of heaviness to the arm specifically on the inside of the arm down toward the small finger. The hand may have tingling and numbness to the tips of the fingers and with aching or throbbing to the inside of the arm near the elbow. The arm may be more painful at night and after activities that either requires sustained bending of the elbow or with repetitive bending of the elbow.
This content was created using EBSCO’s Health Library
Non-operative treatment
Conservative treatment is highly effective for improving symptoms of pain and numbness/tingling to the hand. The physician may recommend use of non-steroidal anti-inflammatory medication as well as rested postures for the elbow. The physician will likely refer you to the physical therapist for education and training in safe positioning of the elbow during repetitive and sustained bending tasks. The therapist will perform an ergonomic evaluation of daily tasks like sleeping, driving, talking on the phone, recreational tasks and work demands. The therapist may suggest a soft brace to wear at night to reduce nighttime bending and may recommend reducing direct pressure by using a pad during the day.
Surgical treatment
If the cubital tunnel has not responded to conservative treatment within a 3-6 month period and there is significant data to show chronic compression, the physician may recommend surgery. Post-operative symptom relief occurs in approximately 93% of patients. Surgical techniques range from in-situ releases of a compressive ligament to transposition of the nerve under protective muscle.
This content was created using EBSCO’s Health Library
If you do have to have surgery, the therapist will follow a specific protocol for safe recovery. Depending on whether the nerve has been moved out of its original location, it will require specific techniques to reduce compression and strain while the nerve is healing. As the soft tissues heal, the nerve can begin to heal as well. After sustained compression for a long period of time, the nerve may have actual damage and needs time to regenerate the nerve sheath and the nerve, itself.
This content was created using EBSCO’s Health Library
Prevention of nerve compression at the elbow requires attention to reducing sustained or repetitive bending, direct compression or trauma. As symptoms begin at the workplace or in daily or recreational tasks, modifications to your tasks may prevent them from getting worse. A physical therapist can guide you toward the modifications that you will need to make to reduce the risk of a chronic condition.
This content was created using EBSCO’s Health Library
- Bayrakli F, Kurtuncu M, Karaarslan E, Ozgen S. (2012). Perineural cyst presenting like cubital tunnel syndrome. Eur spine; Jun 21Dressendorfer R, Richman S. (2012). Cubital tunnel syndrome. CINAHL Rehab Guide; June 01.
- Day CS, Makhni EC, Mejia E, Lage DE, Rosental TD. (2010). Carpal and cubital tunnel syndrome: Who gets surgery? Clinc Orthop Relat Res; Jul:468(7):1796-803.
- Dressendorfer R, Richman S. (2012). Ulnar nerve entrapment syndrome. CINAHL Rehab Guide;Jan 27.
- Gokay NS, Bagatur AE. (2012). Subcutaneous anterior transposition of the ulnar nerve in cubital tunnel syndrome. Acta Orthop Traumatol Turc; 46(4):243-9.
- Thatte MR, Mansukhani KA. (2011). Compressive neuropathy in the upper limb. Indian J Plast Surg; 44(2):283-97.
- Woiewnik B, bindra R. (2009). Cubital tunnel syndrome: Review of current literature on causes, diagnosis and treatment. J Hand Micosurgery; Dec:1(2):76-81.
- Zarezadeh A, Shemshaki H, Nourbaksh M, Etemadifar MR, Moeini M, Mazoochian F. (2012). Comparison of anterior subcutaneous and submuscular transposition of ulnar nerve in treatment of cubital tunnel syndrome: A prospective randomized trial. J red Med Sci; Aug17(8):745-9.
This content was created using EBSCO’s Health Library