Shoulder Dislocation
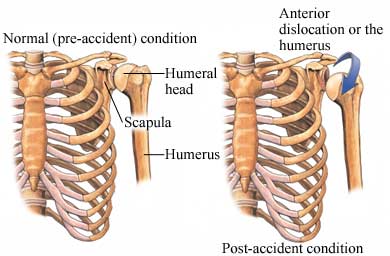
A shoulder dislocation occurs when the head of the humerus (upper arm bone) pops out of the shallow shoulder socket of the scapula (called the glenoid). This can happen when a strong force pulls the shoulder upward or outward, or from an extreme external rotation of the humerus.
Glenohumeral dislocations are generally classified by the direction of dislocation of the humerus.
Dislocation can be full or partial:
• Partial dislocation (also called subluxation)—the head of the humerus slips out of the socket momentarily and then snaps back into place
• Full dislocation—the head of the humerus comes completely out of the socket
Shoulder dislocations can also be associated with fractures—one can have a fracture and dislocation at the same time. Nerves and blood vessels can sometimes be injured with a severe shoulder dislocation, requiring immediate medical attention.
Copyright © Nucleus Medical Media, Inc.
This content was created using EBSCO’s Health Library
Shoulder dislocation can be caused by:
- Falling on an outstretched arm
- A direct blow to the shoulder area, such as in automobile accident
- Forceful throwing, lifting, or hitting
- Force applied to an outstretched arm, such as in a football tackle
This content was created using EBSCO’s Health Library
A risk factor is something that increases your chance of getting a disease, condition, or injury. Risk factors for a shoulder dislocation include:
- Previous shoulder dislocation or subluxation
- Participating in contact sports such as football, wrestling, or hockey
- Conditions involving loose joints, such as Ehlers-Danlos syndrome
- Poor muscle tone
This content was created using EBSCO’s Health Library
Symptoms include:
- Pain, often severe
- Instability and weakness in the shoulder area
- Inability to move the shoulder
- Swelling
- Bruising
- Shoulder contour appears abnormal
- Numbness and tingling around the shoulder or in the arm or fingers
This content was created using EBSCO’s Health Library
The doctor will ask about your symptoms and how the injury occurred, and will examine the injured area. Diagnosis is also based on the physical exam of your shoulder area. The doctor may do an x-ray to rule out a related fracture or damaged surrounding soft tissue and to see in which direction the shoulder is dislocated.
This content was created using EBSCO’s Health Library
After a shoulder dislocation, there are a few important considerations:
- Were other structures damaged? It is very likely that there was a tear of the rotator cuff, a group of muscle-tendon units that move the arm through its range of motion. There might also be a tear of the glenoid labrum, the structure that extends around the glenoid socket, expanding the amount of surface contact between the ball and socket. If the rotator cuff was torn in the dislocation it will probably need to be surgically repaired.
- Your surgeon may place the arm in a sling. There are alternate views behind whether the shoulder should be kept in internal rotation or external rotation in the sling. Internal rotation refers to the position normally seen in slings: the arm is positioned against the body. Recent literature shows that the external rotation position (where the elbow is at the side of the body but the hand in turned out and away from the body) may reduce the tension on the torn ligaments. In a young athlete, the position may be a more important factor. Note, however, that the commonly used abduction sling (with the elbow held away from the body) is specifically for a rotator cuff tear and is not often safe for use with a dislocated shoulder.
NON-SURGICAL shoulder dislocation rehabilitation
- You will probably need to immobilize the shoulder for 1-2 weeks (3-4 weeks for kids and adolescents) depending on the physician’s recommendation. When it is time to move, the physical therapist will focus on gentle active and assisted motion that protects the injured ligaments at the front of the shoulder. It is widely held that passive motion or forcing the shoulder to move can be a dangerous technique following a dislocation. The therapist will likely educate you on the unsafe postures of the shoulder (with the arm up and to the side, elbow bent, and the elbow pointed away from the body). This is called the elevated external rotation position and it is commonly the position that caused the original injury. The therapist will work with you on developing a home exercise program for strengthening the surrounding muscles. Remember that the ligaments can only strengthen due to healing. They are not muscles or attached to muscles so they do not get stronger from strengthening. The muscles can protect the ligaments during the healing process. Be sure to do your home exercise program and do not return to sports or heavy activity without permission from your therapist and physician. Following the instructions will reduce your risk of recurrence.
SURGICAL shoulder dislocation rehabilitation
- If the shoulder has to have surgery after dislocation it is likely in order to repair torn structures. The rotator cuff may have been torn, a nerve may have been pinched, or a ligament may have been completely ruptured off the bone. Each of these surgeries will have a specific protocol for rehabilitation. Furthermore, the shoulder could have frequent dislocations, suggesting that the ligaments never healed after the first injury and are unlikely to heal tightly enough to protect the joint. Some research says that recurrence of dislocation reaches 75% in 20-30 year olds and 30% in 30-40 year olds. The physician will discuss with you the structures that need to be repaired and the level of immobilization needed after the surgery.
This content was created using EBSCO’s Health Library
To help prevent a shoulder dislocation:
- Do exercises to strengthen the muscles around your shoulder.
- Wear proper safety equipment and padding for protection in sports.
- Avoid falls.
This content was created using EBSCO’s Health Library
This content was created using EBSCO’s Health Library
RESOURCES:
- American Academy of Orthopaedic Surgeons
http://www.aaos.org/
- The American Orthopaedic Society for Sports Medicine
http://www.sportsmed.org
CANADIAN RESOURCES:
- Canadian Orthopaedic Association
- Canadian Orthopaedic Foundation
http://www.canorth.org/
REFERENCES:
- American Academy of Orthopaedic Surgeons website. Available at: http://www.aaos.org . Accessed July 9, 2009.
- Quillen DM, Wuchner M, Hatch RL. Acute shoulder injuries. Am Fam Physician. 2004;15;70:1947-1954.
- Shoulder problems. National Institute of Arthritis and Musculoskeletal and Skin Diseases website. Available at: http://www.niams.nih.gov/ . Published 2006. Accessed July 9, 2009.
- Bishay V, Gallo RA. The evaluation and treatment of rotator cuff pathology.
- Prim Care. 2013 Dec;40(4):889-910, viii.
- Lynch E, Lombard J, Coopoo Y, Shaw I, Shaw B. Shoulder injury incidence and severity through identification of rugby union players. Pak J Med Sci. 2013 Nov;29(6): 1400-5.
- Atalar AC, Bilsel K, Eren I, Celik D, Cil H, Demirhan M. Modified latarjet procedure for patients with glenoid bone defect accompanied with anterior shoulder instability. Acta Orthop Traumatol Turc. 2013;47(6):393-9Choose Destination.
- Ji JH, Shafi M, Park SE, Park PY. A severly displaced metaphyseal fracture of the proximal humerus with dislocation of the shoulder in a child. Chin J Traumatol. 2014 Feb 1;17(1):54-6.
- Nitz AJ. Special issue: Shoulder complex: Physical therapy management of the shoulder.Phys Ther. 1986 Dec;66 (1912-1919).
- McClure PW, Flowers KR. Special Issue: Manual Therapy: Treatment of Limited Shoulder Motion: A Case Study Based on Biomechanical Considerations. Phys Ther. 1992 Dec;72.
This content was created using EBSCO’s Health Library