Diabetes (Type 1)
Diabetes is a higher level of glucose in the blood than is normal. Glucose travels through your body in the blood. A hormone called insulin then helps glucose move from your blood to your cells. Once glucose is in your cells it can be used for energy. A problem making or using insulin means glucose cannot move into your cells. Instead the glucose will build up in your blood.
In type 1 diabetes, the body does not make insulin. This will lead to the build up of glucose in the blood, also called hyperglycemia. At the same time, your cells are not getting glucose they need to function well. Over a long period of time, high blood glucose levels can also damage vital organs. The blood vessels, heart, kidneys, eyes, and nerves are most commonly affected organs.
Type 1 diabetes is often found during childhood and young adulthood.
Copyright © Nucleus Medical Media, Inc.
This content was created using EBSCO’s Health Library
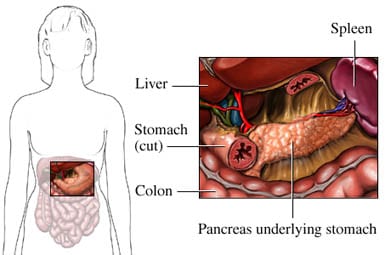
Our immune system keeps us healthy by fighting off and destroying viruses and bacteria. Unfortunately, sometimes the immune system attacks healthy tissue. Most commonly, type 1 diabetes develops because the immune system attacks and destroys the cells that make insulin. These cells are in the pancreas. It is not yet clear why the immune system attacks these cells. It is believed that some people have genes that make them prone to getting diabetes. For these people, certain triggers in the environment may make the immune system attack the pancreas. The triggers are not known but may be certain viruses, foods, or chemicals. Type 1 diabetes may also develop as a complication of other medical conditions. It may develop in:
- People with chronic type 2 diabetes who lose the ability to make insulin.
- Some with chronic pancreatitis or pancreatic surgery. They may lose the cells that make insulin.
This content was created using EBSCO’s Health Library
Risk factors include:
- Family history (parent, sibling) of type 1 diabetes
- Age: starts as early as age 4 with peak at ages 11-13
- Sex: more common in males than females
- Ethnicity: Northern European, Mediterranean, African American, Hispanic
- Increased age of mother during pregnancy
- Increased birth weight
- Obesity during childhood
- Other autoimmune illness, including:
- Hashimoto’s disease —disease of the thyroid
- Graves’ disease —disease of the thyroid
- Addison’s disease —disorder of the adrenal glands
- Pernicious anemia
- Celiac disease —autoimmune disease of the digestive tract
- Vitiligo —disorder that affects the skin cells
- Cystic fibrosis
This content was created using EBSCO’s Health Library
If you have any of these symptoms, do not assume it is due to type 1 diabetes. These symptoms may be caused by other conditions. Tell your doctor if you have any of these:
- Weight loss
- Increased urination
- Extreme thirst
- Hunger
- Fatigue, weakness
- Blurry vision
- Irritability
- Headaches
Without insulin, your body will need to find new forms of energy. This will cause an imbalance in the body called ketoacidosis. It is a severe state that can lead to coma or death. Symptoms of ketoacidosis include:
- Vomiting and nausea
- Abdominal pain
- Dehydration (not enough fluid in the body)
- Drowsiness
- Abnormally deep and fast breathing
- Coma
- Dry skin and mouth
- Fruity breath odor
- Rapid pulse
- Low blood pressure
This content was created using EBSCO’s Health Library
The doctor will ask about your symptoms. You will also be asked about your medical and family history. A physical exam will be done. Type 1 diabetes is diagnosed based on the results of blood tests and other criteria. These include:
- Symptoms common with diabetes and a random blood test showing a blood sugar level greater than or equal to 200 mg/dL* (11.1 mmol/L)
- Fasting blood test showing blood glucose levels greater than or equal to 126 mg/dL (7.0 mmol/L) on two different days—the test is done after you have not eaten for eight or more hours
- Glucose tolerance test results with blood glucose greater than or equal to 200 mg/dL (11.1 mmol/L)—test is done after you eat glucose
- HbA1c level of 6.5% or higher—measure of blood sugar over the past 2-4 months
*mg/dL = milligrams per deciliter of blood, mmol/L = millimole per liter of blood You may also need other blood tests to confirm diabetes is type 1 and not type 2. These may include:
- Insulin level or C-peptide tests—to see how much insulin is being made by the pancreas
- Tests that look for antibodies that are working against your pancreas
This content was created using EBSCO’s Health Library
Treatment aims to:
- Maintain blood sugar at levels as close to normal as possible
- Maintain a healthy weight
- Prevent or delay complications
- Control other conditions that you may have, like high blood pressure and high cholesterol
After an initial evaluation your physical therapy will be able to create a rehabilitation program designed to meet your goals. It is important to remain in close contact with your physician – a change may need to be made to your insulin dose or diet if you are having low glucose levels after exercise. A physical therapist can also help with certain complications of Diabetes such as Diabetic Neuropathy (covered in the foot section of the injury center). Your physical therapy program may include:
- Aerobic exercises & resistance training: Both types of exercise help to improve long-term glucose control. Regular exercise can also help reduce your risk of heart disease.
- Patient education & information on exercise precautions
This content was created using EBSCO’s Health Library
Currently, there is no known way to prevent type 1 diabetes. Some research is looking at the effectiveness of suppressing the immune system. This may be helpful in people who are at high risk of developing type 1 diabetes.
This content was created using EBSCO’s Health Library
This content was created using EBSCO’s Health Library
RESOURCES:
- American Diabetes Association
http://www.diabetes.org/
- National Diabetes Information Clearinghouse
http://diabetes.niddk.nih.gov/
CANADIAN RESOURCES:
- Canadian Diabetes Association
http://www.diabetes.ca/
- Team Diabetes Canada
- Canadian Diabetes Association
http://www.diabetes.ca/
REFERENCES:
- American Association of Clinical Endocrinologists. American College of Endocrinology. Medical guidelines for the clinical practice for the management of diabetes mellitus. Endocrine Pract . 2007;13(suppl 1)3-68.
- American Association of Clinical Endocrinologists. American College of Endocrinology. Medical guidelines for the management of diabetes mellitus: the AACE system of intensive diabetes self-management. 2002 update. Endocrine Pract . 2002;8(suppl 1)S40-82.
- The DCCT/Epidemiology of Diabetes Interventions and Complications Research Group. Retinopathy and nephropathy in patients with type 2 diabetes four years after a trial of intensive therapy. N Engl J Med . 2000;342:381-389.
- Diabetes. National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/nccdphp/publications/aag/ddt.htm . Updated February 14, 2008. Accessed July 21, 2008.
- Diabetes causes. National Institute of Diabetes & Digestive & Kidney Diseases website. Available at: http://www.niddk.nih.gov/ . Accessed December 31, 2012.
- Diabetes type 1. EBSCO DynaMed website. Available at: http://www.ebscohost.com/dynamed/what.php . Updated December 28, 2012. Accessed December 31, 2012.
- Paviakis M, Khwaja K. Pancrease and islet cell transplantation in diabetes. Curr Opin Endocrinol Diabetes Obes . 2007;14:146-150.
- Physical activity/exercise and diabetes. Diabetes Care . 2004;27(suppl 1)S58-62.
- Traina AN, Kane MP. Primer on pramlintide, an amylin analog. Diabetes Educ. 2011;37(3):426-431.
- Type 1 diabetes. American Diabetes Association website. Available at: http://www.diabetes.org/ . Accessed December 31, 2012.
- 9/23/2008 DynaMed’s Systematic Literature Surveillance http://www.ebscohost.com/dynamed/what.php : The Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group. Continuous glucose monitoring and intensive treatment of type 1 diabetes. N Engl J Med. 2008 Sep 8. [Epub ahead of print]
- 3/12/2010 DynaMed’s Systematic Literature Surveillance http://www.ebscohost.com/dynamed/what.php : Cardwell CR, Stene LC, Joner G, et al. Birthweight and the risk of childhood-onset type 1 diabetes: a meta-analysis of observational studies using individual patient data. Diabetologia. 2010 Jan 10. [Epub ahead of print]
- 4/1/2011 DynaMed’s Systematic Literature Surveillance http://www.ebscohost.com/dynamed/ : Verbeeten KC, Elks CE, Daneman D, Ong KK. Association between childhood obesity and subsequent Type 1 diabetes: a systematic review and meta-analysis. Diabet Med. 2011;28(1):10-18.
This content was created using EBSCO’s Health Library